
Physical Activity Offers a Critical Window to Mitigate Immediate Dietary Damage to Arteries.
In an era increasingly defined by convenience and readily available processed foods, a compelling body of research highlights a critical, albeit temporary, window where physical activity can help mediate some of the acute physiological damage inflicted by an unhealthy meal. This scientific insight underscores the profound, almost immediate, impact of diet on our cardiovascular system and the surprising power of timely exercise to counteract adverse effects. The findings serve as a stark reminder of the dynamic interplay between lifestyle choices and arterial health, moving beyond long-term consequences to reveal instantaneous changes within the human body.
The Immediate Assault on Arterial Function from High-Fat Meals
Previous studies have meticulously documented how a single meal rich in saturated fat can significantly impair arterial function. While initial observations focused on peripheral arteries, such as those in the arm, the implications for critical blood flow to the heart wall are far more concerning. Researchers have conducted randomized trials to investigate these effects, typically by comparing the impact of high-fat meals against low-fat alternatives. One such study involved men consuming either a meal where over 60% of calories came from fat, half of which was saturated, and containing a substantial amount of cholesterol (exceeding that in a single egg), or a control meal that was predominantly carbohydrate-based, with less than 10% fat and significantly lower cholesterol levels—a stark 50-fold difference.
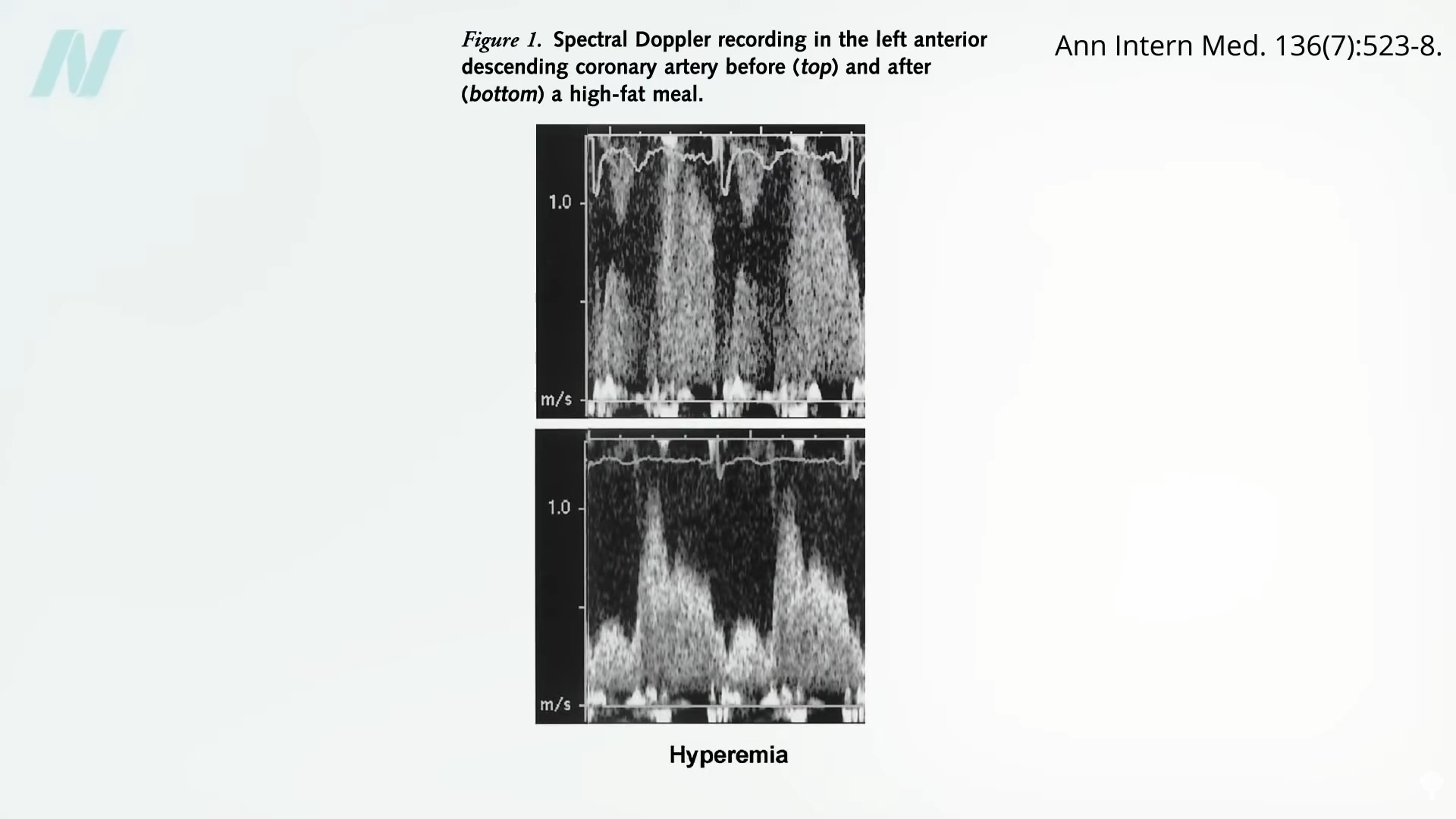
The results of these investigations are visually striking and physiologically significant. Doppler recordings of the left anterior descending coronary artery, often colloquially referred to as the "widow-maker" due to its critical role in supplying blood to the heart, provide undeniable evidence. Before a high-fat meal, the artery typically exhibits a strong, clear signal, indicative of healthy blood flow. Within mere hours of consuming such a meal, this robust signal can be seen to diminish dramatically, indicating a constriction or impairment of blood flow. For instance, recordings taken just five hours post-consumption often reveal a significantly squeezed signal, demonstrating the rapid physiological response to dietary fat.
Beyond mere constriction, high-fat meals profoundly affect what is known as coronary flow reserve. This vital physiological capacity refers to the heart’s ability to increase blood flow when needed, particularly when a part of a coronary artery is blocked. In such scenarios, surrounding vessels typically expand to compensate, ensuring adequate oxygen supply to the heart muscle. However, studies show that after a single high-fat meal, this crucial coronary flow reserve is clamped down. This acute impairment undermines the heart’s inherent ability to adapt and compensate for potential blockages, thereby increasing vulnerability to cardiac events. Crucially, this reduction in coronary flow reserve was observed only after high-fat meals, not after calorically equivalent low-fat meals, highlighting the specific detrimental role of dietary fat composition.

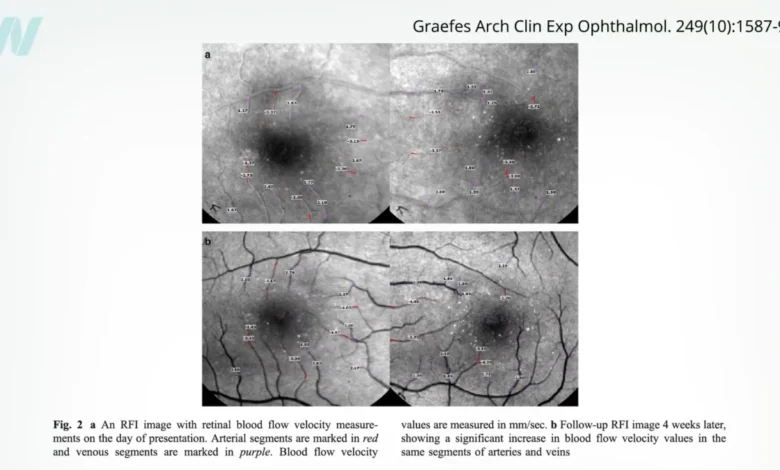
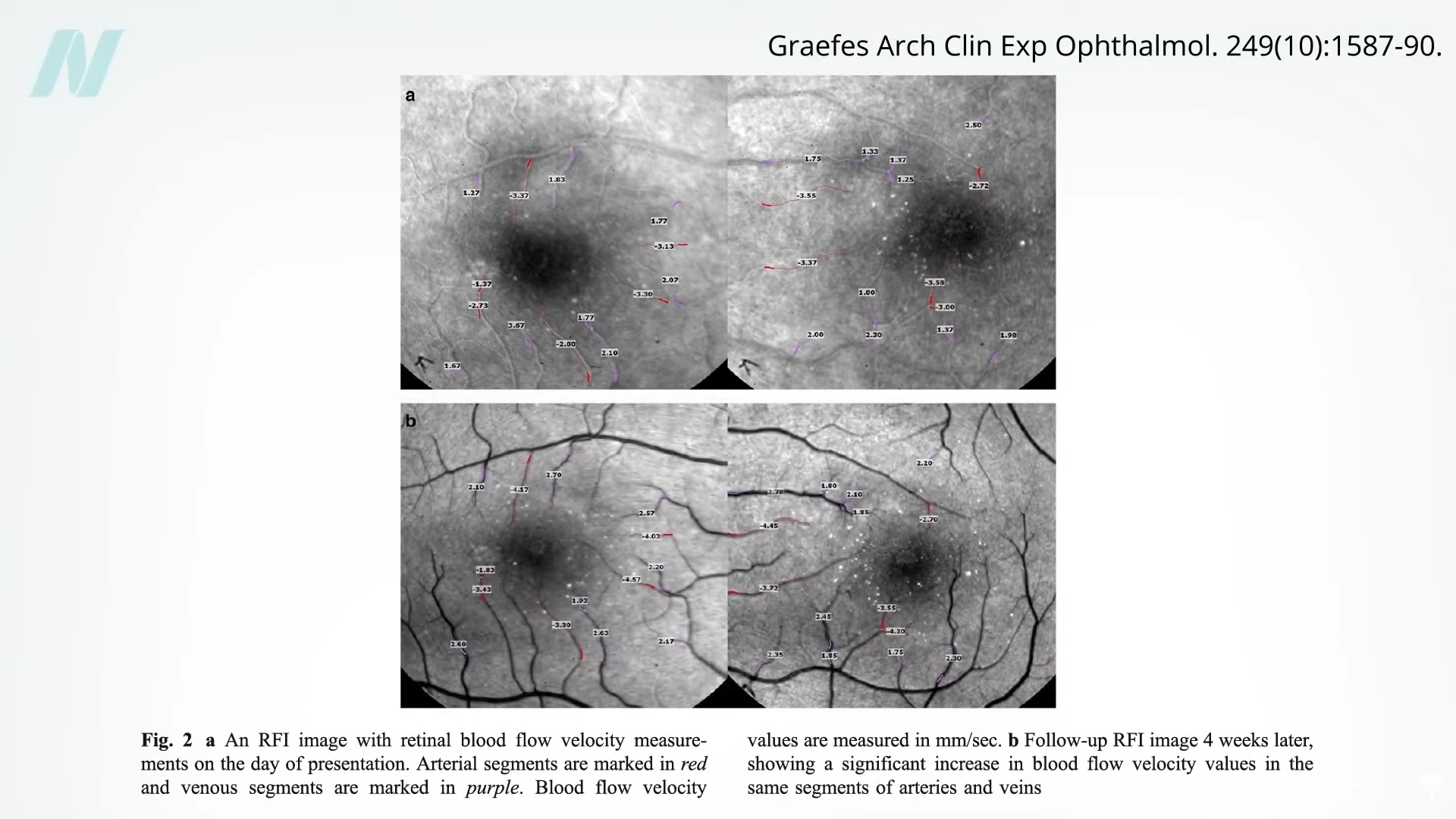
The systemic impact of such meals extends beyond the heart. In extreme instances, the effects of high postprandial lipemia—the elevated fat levels in the blood after a meal—can even be observed in the delicate vasculature of the retina. Before-and-after images of a patient’s retina can dramatically illustrate this phenomenon. Initial images might show milky-colored blood vessels, indicative of significant fat accumulation in the bloodstream, sometimes described as blood resembling a "milkshake." Following interventions such as a low-fat diet and medication to clear fat from the bloodstream, subsequent images reveal a noticeable clearing of these vessels, underscoring the direct and pervasive influence of dietary fat on microvascular health throughout the body.
The Timely Intervention: Exercise as a Mitigating Factor
The immediate adverse effects of high-fat meals on arterial function naturally lead to the question of mitigation. Can exercise, known for its myriad long-term cardiovascular benefits, offer an acute protective effect? Research suggests a promising "yes," but with specific timing considerations. Post-meal inflammation and the extended elevation of fats (lipemia) in the blood after high-fat meals are strongly implicated in increasing cardiovascular disease risk. However, substantial evidence now indicates that acute exercise can be an effective strategy to accelerate the clearance of these fats from the bloodstream.
The beneficial effects of acute exercise on postprandial lipemia appear to be relatively short-lived, emphasizing the importance of consistent activity. Going even a few days without exercise can negate any prior benefits, irrespective of an individual’s overall fitness level. The crucial time window for this protective effect spans approximately 18 hours before the high-fat meal and extends to about 90 minutes after consumption. Within this window, engaging in physical activity can significantly reduce the acute damage. The recommended duration and intensity appear to be around an hour of moderate-intensity exercise. This could include brisk walking, cycling, or other activities that elevate heart rate and breathing without being exhaustive.
A particularly insightful study demonstrated the practicality of this concept using a common, notoriously unhealthy meal: a McDonald’s breakfast consisting of hash browns, eggs, pancakes, an English muffin, sausage, and a milkshake. This calorically dense and nutrient-poor meal, laden with fat and sodium, typically leads to a significant decrease in artery function when individuals remain sedentary afterwards. However, the study found that just 20 minutes of stair climbing, broken into five-minute intervals performed every hour for four hours after the meal, was sufficient to attenuate these negative effects. In the group that performed these hourly "exercise snacks," artery function did not significantly decrease. This suggests that incorporating brief, hourly bouts of activity, such as stair climbing, can serve as an easily accessible lifestyle strategy to protect vascular function, mitigating the immediate harm from indulgent meals and prolonged sitting. While exercise offers a buffer, it is crucial to note the obvious alternative: avoiding such high-fat, high-sodium meals in the first place remains the most effective strategy for arterial health.
The Insidious Threat of Sodium: Beyond Blood Pressure
Beyond fat, the sodium content in many processed and fast foods presents another significant, often underestimated, threat to arterial health. The aforementioned McDonald’s breakfast, for instance, can contain over 2,000 mg of sodium—exceeding the American Heart Association’s (AHA) recommended daily limit of 1,500 mg for most adults. Research indicates that even a single meal with high sodium content, such as one containing 2,000 mg or even a third less, can impair artery function within an hour of consumption. This impairment occurs independently of an increase in blood pressure, highlighting a direct effect of sodium on vascular health that is often overlooked.
The conventional understanding of sodium’s impact on health primarily revolves around its role in hypertension. Some individuals are classified as "salt-sensitive," experiencing a significant spike in blood pressure with high sodium intake, while others are deemed "salt-resistant," showing minimal blood pressure fluctuations. However, recent findings challenge the notion that salt is acceptable for "salt-resistant" individuals. Studies unequivocally demonstrate that high dietary sodium intake reduces artery function regardless of an individual’s blood pressure sensitivity to salt. Whether one is salt-sensitive or salt-resistant, transitioning from a low-salt to a high-salt diet impairs artery function, underscoring a pervasive and universal vascular vulnerability to excessive sodium. Visual representations, such as Doppler measurements, clearly illustrate this decline in arterial function even in individuals whose blood pressure remains stable.
This evidence points to an influence of dietary salt that extends beyond mere blood pressure regulation. High sodium intake can induce endothelial dysfunction, increase oxidative stress, and promote inflammation within the arterial walls, all of which contribute to impaired vascular health even without a noticeable rise in systemic blood pressure. Despite a seemingly unanimous scientific consensus on the detrimental effects of excessive sodium, a vocal minority of researchers, often with industry funding connections, continue to claim that reducing salt intake is unnecessary or even harmful. However, the overwhelming scientific evidence stands firm against these dissenting voices. Much like the saturated fats found in meat, dairy, and ultra-processed junk foods, sodium—not its reduction—is consistently identified as the true "villain" in the context of cardiovascular health.
Broader Implications and Public Health Imperatives
The immediate and profound impacts of high-fat and high-sodium meals on arterial function, coupled with the mitigating potential of timely exercise, carry significant implications for public health and individual lifestyle choices. In a society grappling with rising rates of cardiovascular disease, understanding these acute physiological responses is crucial. It moves the conversation beyond long-term, cumulative damage to highlight the daily, even hourly, consequences of dietary choices.
These findings reinforce the paramount importance of preventive nutrition. Prioritizing whole, unprocessed foods that are naturally low in saturated fat and sodium remains the cornerstone of cardiovascular health. Reducing the consumption of fast food and highly processed items is not merely a recommendation for long-term well-being but an immediate protective measure against acute arterial impairment.
However, for those instances where unhealthy meals are consumed, the research offers a practical, albeit temporary, compensatory strategy. The concept of "exercise snacks" or a dedicated moderate-intensity workout within the identified time window can serve as a vital tool to lessen the immediate physiological burden. This is particularly relevant in modern sedentary lifestyles, where prolonged sitting further exacerbates the negative effects of poor diet. Integrating brief bursts of physical activity into daily routines, especially around meal times, could represent a powerful, accessible intervention.
Public health initiatives and dietary guidelines must continue to emphasize both the reduction of harmful dietary components (saturated fat, sodium) and the promotion of regular physical activity. Education campaigns can highlight the immediate consequences illustrated by these studies, making the abstract concept of "heart health" more tangible and urgent. Policymakers can support environments that make healthy food choices more accessible and physical activity more feasible.
Ultimately, while exercise offers a valuable acute protective mechanism, it is not a license to consistently indulge in unhealthy eating. The cumulative effect of frequent high-fat, high-sodium meals, even if occasionally mitigated by exercise, will still likely contribute to long-term arterial damage and increased cardiovascular risk. The scientific evidence consistently points towards a holistic approach: making conscious, healthful dietary choices as a primary defense, complemented by consistent physical activity, to safeguard arterial function and promote lasting cardiovascular wellness.
This discussion is part of a series delving into the intricate relationship between diet, saturated fat, and artery health. The initial segment explored "How a Single Meal Can Cripple Your Arteries and Lungs," setting the stage for understanding immediate physiological impacts. The upcoming segment will further enrich this understanding by focusing on specific foods that can actively protect arteries from the detrimental effects of saturated fat. For those seeking deeper insights into the pervasive dangers of sodium, comprehensive research on "The Evidence That Salt Raises Blood Pressure" offers additional critical perspectives.







{kind=link}