
New research highlights simple yet effective dietary interventions involving broccoli, vinegar, and lemon juice in the effort to mitigate the glycemic impact of white potatoes. These common kitchen staples are being put to the test as accessible tools to help regulate blood sugar responses, offering promising insights for individuals concerned about metabolic health. The findings suggest that while white potatoes inherently possess a high glycemic index (GI), their consumption doesn’t necessarily have to lead to detrimental health outcomes if paired with the right accompaniments.
Understanding the Glycemic Challenge of White Potatoes
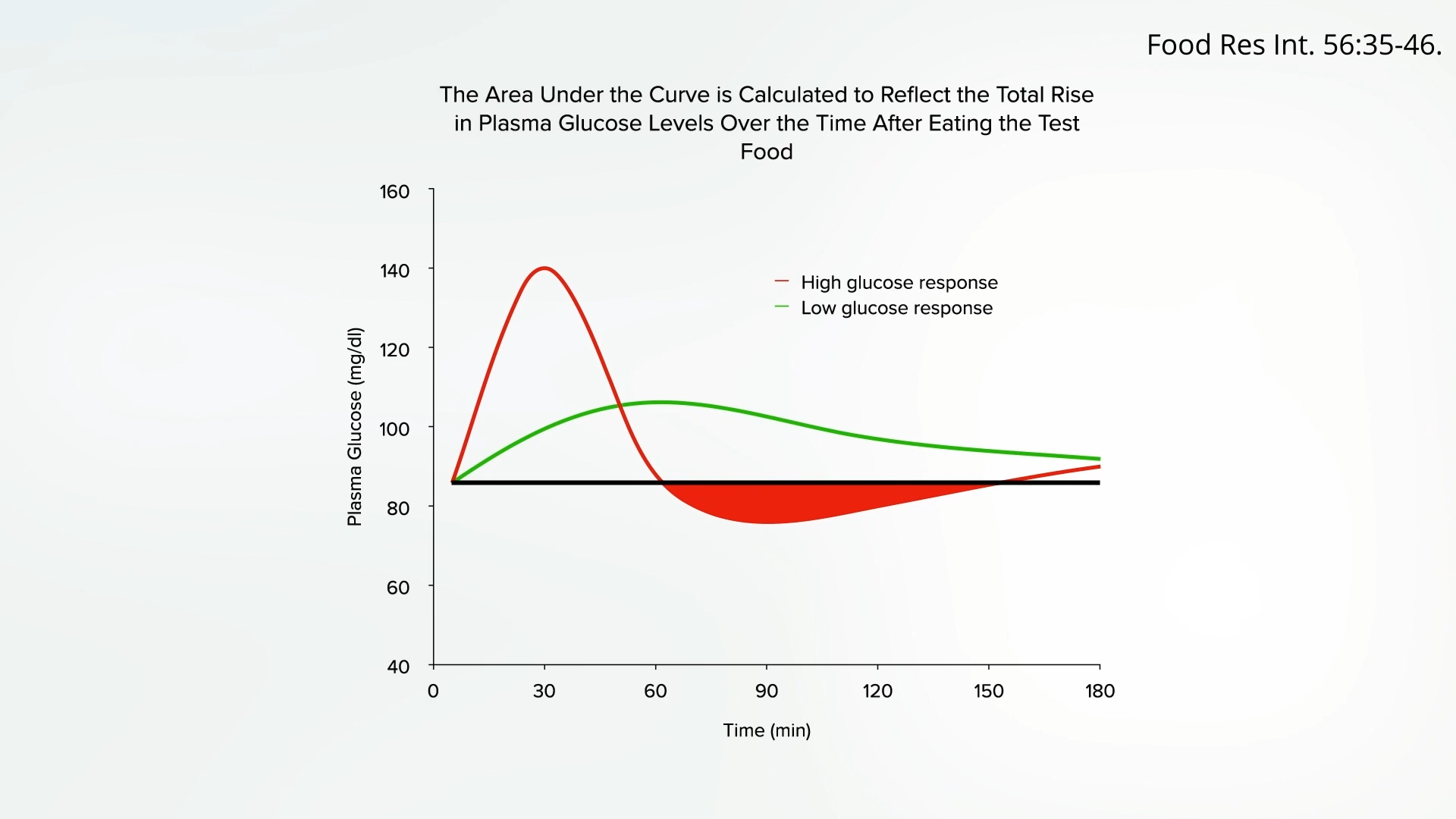
White potatoes have long been a dietary staple across cultures, prized for their versatility and nutritional content. However, their classification as a high glycemic index food has raised concerns among health professionals and individuals managing conditions like diabetes. The glycemic index is a system that ranks carbohydrate-containing foods by how much they raise blood sugar levels after eating. Foods with a high GI are rapidly digested and absorbed, leading to a quick and pronounced spike in blood glucose.
Normally, after consuming a meal, the body’s blood sugar levels should rise and fall gently and naturally. This controlled fluctuation allows for efficient energy distribution and utilization. In contrast, high-GI foods like white potatoes can trigger an exaggerated blood sugar surge. This rapid increase prompts the pancreas to release an excessive amount of insulin to bring blood glucose back down. This over-compensation can lead to blood sugar levels dropping lower than their pre-meal baseline, a phenomenon known as reactive hypoglycemia. Such dramatic fluctuations are not merely uncomfortable; they can instigate a cascade of negative metabolic consequences, including an increase in triglyceride fats in the blood, which is a risk factor for cardiovascular disease. The physiological mechanism involves the liver converting excess glucose into triglycerides when insulin levels are high, especially after a rapid influx of carbohydrates. This metabolic strain, if chronic, contributes significantly to insulin resistance and the progression towards type 2 diabetes.
Despite these glycemic challenges, it is crucial to acknowledge that white potatoes are not devoid of nutritional value. They are a good source of essential micronutrients, including vitamin C, which is vital for immune function and collagen synthesis, and potassium, an electrolyte crucial for blood pressure regulation and nerve function. Furthermore, potatoes contain beneficial polyphenols, a type of antioxidant that may offer protective effects against various diseases. This nutritional profile might explain why, in broader epidemiological studies, potatoes appear to have a neutral effect on lifespan, unlike other whole plant foods that have been more directly associated with actively living longer. The interplay of their high carbohydrate load and beneficial micronutrients presents a complex nutritional picture, prompting researchers to seek strategies to maximize their benefits while minimizing their drawbacks.

Prior Interventions: The Science of Chilling and Resistant Starch
Before delving into the recent findings on broccoli, vinegar, and lemon juice, it’s important to recall previous insights into modifying potato’s glycemic impact. Earlier research highlighted that the simple act of chilling cooked potatoes can dramatically lower their glycemic index. This phenomenon is attributed to the retrogradation of starch. When starchy foods like potatoes are cooked and then cooled, some of the digestible starch converts into resistant starch. Resistant starch, as its name suggests, resists digestion in the small intestine and ferments in the large intestine, behaving much like dietary fiber. This process slows down glucose absorption, resulting in a more gradual and sustained release of sugar into the bloodstream, thereby blunting the post-meal blood sugar spike. Remarkably, this beneficial effect persists even if the chilled potatoes are subsequently reheated, making it a practical strategy for meal preparation and consumption. This discovery opened avenues for exploring other accessible methods to achieve similar glycemic control.
Novel Approaches: Broccoli, Vinegar, and Lemon Juice
Building on the understanding that dietary modifications can significantly alter the metabolic response to high-GI foods, researchers have turned their attention to common food pairings and condiments. The latest investigations explored the efficacy of broccoli, vinegar, and lemon juice in reducing the glycemic and insulinemic responses to white potatoes.
Intervention 1: The Potent Pairing of Broccoli – Plant vs. Animal Protein
One of the most compelling findings relates to the inclusion of broccoli. Studies indicate that eating just two servings of cooked broccoli alongside mashed potatoes can substantially reduce the body’s insulin demand by nearly 40%. This remarkable effect underscores the power of whole plant foods in modulating metabolic responses. Broccoli, a cruciferous vegetable, is rich in fiber, vitamins, minerals, and various phytochemicals, all of which contribute to its health-promoting properties. The fiber content, in particular, slows down digestion and nutrient absorption, which can help mitigate rapid blood sugar increases. Furthermore, the overall nutritional matrix of broccoli may enhance insulin sensitivity and improve glucose metabolism.
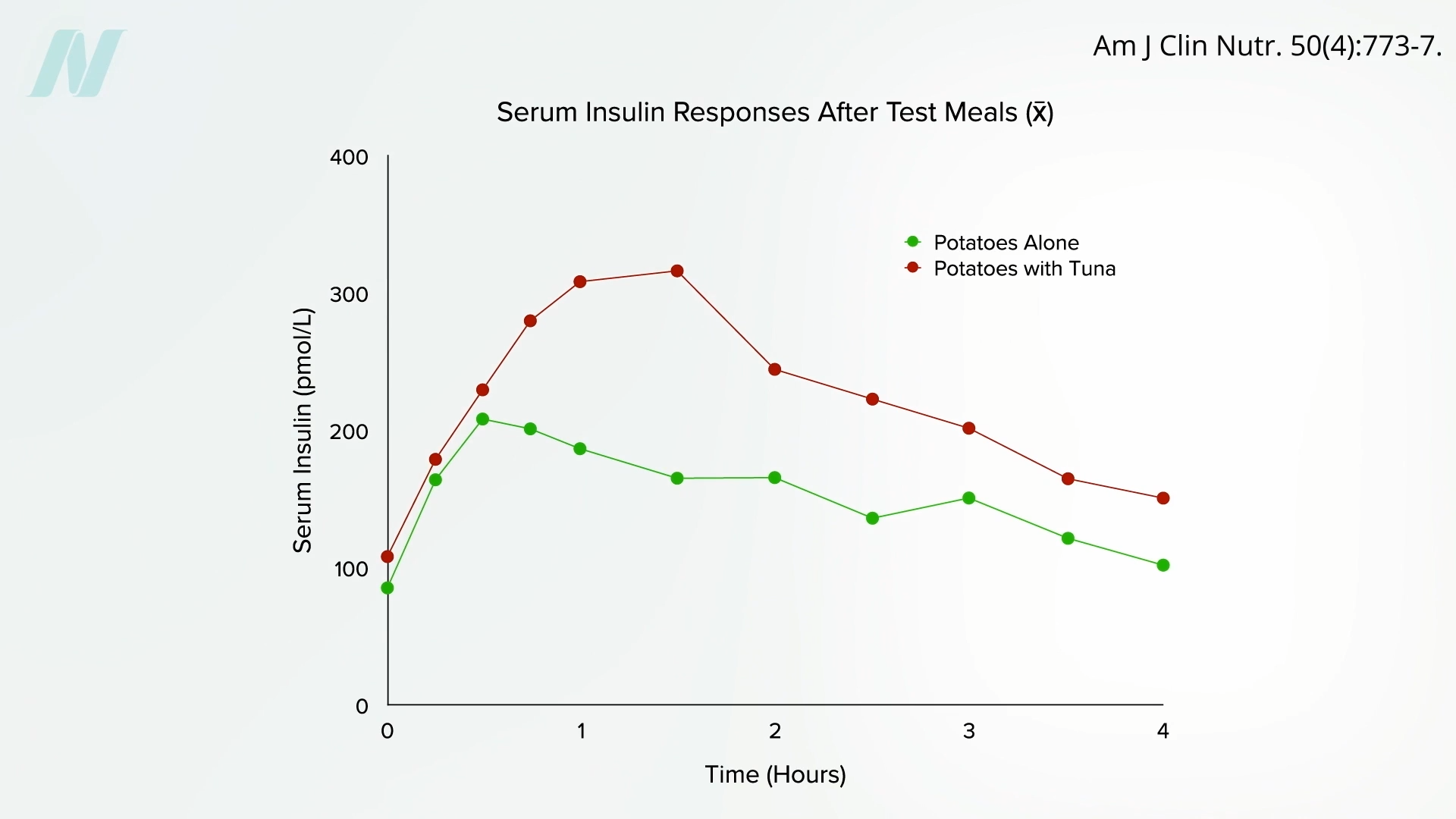
In stark contrast to the beneficial effects of plant-based protein and fiber, the addition of animal proteins like chicken breast or tuna fish to mashed potatoes had a detrimental effect. Consuming chicken breast alongside potatoes worsened the glycemic response, while tuna fish made things even more pronounced, nearly doubling the amount of insulin the body had to pump out. This counterintuitive finding highlights a critical distinction between different protein sources and their metabolic impacts.
The underlying biochemical explanation for this divergence lies in the composition of amino acids. Animal proteins tend to be higher in branched-chain amino acids (BCAAs) such as leucine, isoleucine, and valine. While BCAAs are essential and play roles in muscle protein synthesis, excessive intake, particularly in the context of insulin resistance, has been linked to impaired metabolic health. Research indicates that decreased consumption of BCAAs can improve metabolic health, suggesting that a diet rich in plant-based proteins, which typically have a lower BCAA profile compared to animal proteins, may offer advantages for blood sugar regulation and insulin sensitivity. This insight, explored in detail in works such as "How Not to Diet," provides a crucial piece of the puzzle in understanding why plant-based dietary patterns are consistently associated with better metabolic outcomes. The implication for dietary guidelines is clear: pairing high-GI carbohydrates with whole plant foods, especially those rich in fiber and beneficial compounds, is a superior strategy compared to combining them with animal proteins.
Intervention 2: The Acetic Acid Advantage – Vinegar’s Proven Efficacy
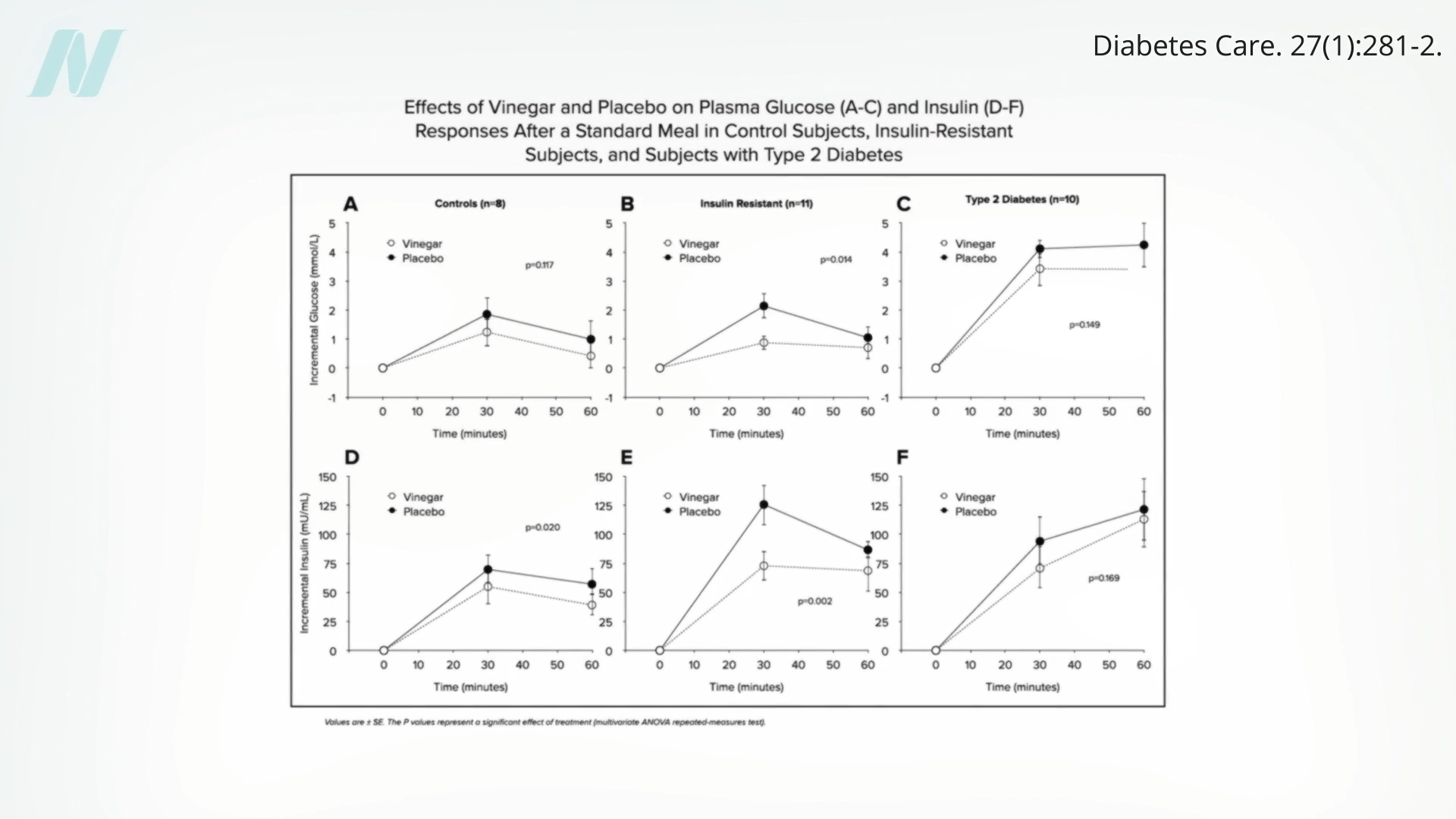
The role of vinegar in glycemic control is not a new discovery, but its application to white potatoes provides further evidence of its widespread utility. The acetic acid in vinegar has been shown to exert significant effects on carbohydrate metabolism. Previous studies, for instance, illustrated how individuals with prediabetes experienced significantly reduced blood sugar and insulin spikes after consuming a bagel alongside a tablespoon of apple cider vinegar diluted in about a quarter cup of water. This effect is attributed to several mechanisms: acetic acid can slow gastric emptying, meaning food stays in the stomach longer, leading to a more gradual release of glucose into the bloodstream. It can also inhibit the activity of certain enzymes responsible for starch digestion in the small intestine, further reducing the rate of glucose absorption.
Applying this principle to potatoes, research confirms that while chilling alone helps, adding approximately a tablespoon of vinegar can lead to even more significant drops in blood sugar and insulin levels, typically ranging from 30% to 40%. This effect was observed even with plain white distilled vinegar, indicating that the active component is likely the acetic acid itself, rather than other compounds specific to particular vinegar types like apple cider vinegar. The accessibility and low cost of vinegar make it an exceptionally practical and scalable intervention for glycemic management.
The implications for public health are substantial. Given vinegar’s potent ability to modulate post-meal glucose responses, clinicians and dietitians may increasingly consider incorporating vinegar consumption as a dietary recommendation for patients with diabetes or prediabetes. Integrating a simple tablespoon of vinegar, diluted in water, into daily routines could provide a non-pharmacological adjunct to conventional glucose management strategies, empowering individuals to take a more active role in their metabolic health.
Intervention 3: Lemon Juice – A Zesty, Acidic Alternative
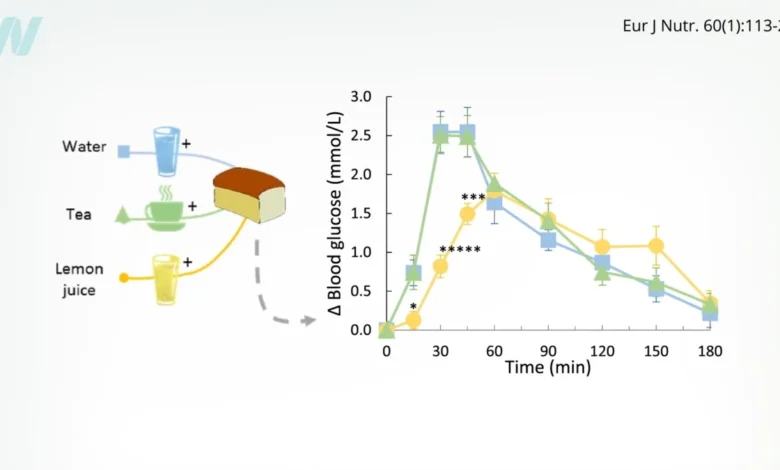
The question naturally arises whether the glycemic-blunting effect is specific to vinegar or if other acidic condiments could yield similar benefits. Initial test-tube studies showed that lemon juice possessed a remarkable starch-blocking effect, suggesting its potential to interfere with carbohydrate digestion. To validate this in human subjects, further research was conducted.
Indeed, lemon juice was found to significantly reduce the glycemic responses to bread. Participants who consumed bread along with lemon juice experienced approximately a 30% reduction in their blood sugar response. What makes this finding particularly noteworthy is that the study participants were drinking about half a cup of lemon juice, which inherently contains a small amount of natural sugars. Despite this added sugar load, the overall blood sugar response was still improved, highlighting the potent starch-blocking and metabolic-modulating properties of lemon juice’s acidic components, primarily citric acid.
While both vinegar and lemon juice demonstrate beneficial effects, comparative analyses suggest that vinegar tends to be more potent. Studies indicate that consuming just one to two tablespoons of vinegar daily, diluted in water, can significantly improve both short-term (post-meal) and long-term (HbA1c) blood sugar control in individuals with diabetes. This robust and consistent effect positions vinegar as a particularly strong candidate for dietary recommendations aimed at glycemic management. However, lemon juice offers a flavorful and versatile alternative, especially for those who may prefer its taste or wish to incorporate acidity in different culinary contexts. The practical application of these findings encourages individuals to use lemon juice liberally in dressings, marinades, or as a condiment to meals containing high-GI carbohydrates.
Broader Impact and Dietary Implications
The cumulative findings regarding chilling, broccoli, vinegar, and lemon juice offer a multifaceted and practical framework for reducing the glycemic impact of white potatoes and, by extension, other high-carbohydrate foods. These simple dietary adjustments provide powerful tools for individuals to enjoy a wider variety of foods while proactively managing their metabolic health.
The implications extend beyond just potatoes. These strategies underscore a broader principle in nutrition: the overall dietary context of a meal profoundly influences its metabolic outcome. It’s not just about the individual food item but how it’s prepared and what it’s eaten with. This paradigm shift encourages a more holistic approach to eating, moving away from strict avoidance of certain foods towards intelligent pairing and preparation.
For individuals at risk of or managing type 2 diabetes, these findings offer empowering, accessible, and non-pharmacological interventions. Integrating these practices into daily eating habits – whether it’s chilling potatoes for a salad, adding a generous serving of broccoli to a meal, or incorporating vinegar-based dressings and lemon juice into cooking – can contribute to better blood sugar control, reduced insulin demand, and ultimately, improved long-term metabolic health. This evidence-based approach provides valuable guidance for nutritionists, dietitians, and healthcare providers to offer nuanced and practical dietary advice tailored to individual needs and preferences.
Looking Ahead: The Ongoing Exploration of Potato Health
This exploration into mitigating the glycemic impact of potatoes is part of a larger, ongoing series of investigations into the health benefits and considerations of this ubiquitous root vegetable. Future research aims to address other common concerns, such as the presence of glycoalkaloid toxins in potatoes and to identify the healthiest types of potatoes based on their overall nutritional profile and metabolic effects. The continuous scientific inquiry into dietary components ensures that nutritional recommendations remain dynamic, evidence-based, and maximally beneficial for public health. These simple, yet powerful, dietary modifications represent significant strides in translating complex nutritional science into actionable advice for everyday eating.





{kind=link}