
Does the link between white potatoes and diabetes extend to non-fried potatoes without butter or sour cream?
The relationship between dietary choices and chronic diseases like Type 2 Diabetes remains a critical area of public health investigation. Among the many food items scrutinized for their potential impact, the humble white potato has frequently found itself at the center of debate. For decades, potatoes have been a staple in diets worldwide, often classified as a vegetable in dietary guidelines. However, a series of influential studies, primarily originating from Harvard University, began to challenge this long-held perception, raising questions about whether even non-fried preparations of potatoes could contribute to an increased risk of Type 2 Diabetes. This inquiry gained significant traction in 2006, marking a pivotal moment in nutritional science.
The Genesis of Concern: Early Harvard Studies and the Nurses’ Health Cohort
The initial alarm regarding white potatoes was sounded in 2006 with the publication of findings from the extensive Harvard Nurses’ Health Study. This groundbreaking research, which meticulously tracked the dietary habits and health outcomes of tens of thousands of women over two decades, concluded that a higher intake of potatoes was significantly associated with a greater likelihood of developing Type 2 Diabetes. The study, published in the American Journal of Clinical Nutrition, utilized a prospective cohort design, a robust methodology allowing researchers to observe participants over time and identify associations between exposures (like diet) and outcomes (like disease).
At the time of this initial study, American potato consumption habits leaned heavily towards processed and deep-fried forms. Data from the United States Department of Agriculture (USDA) indicated that the average American consumed over 100 pounds of potatoes annually, with a substantial portion in the guise of potato chips, french fries, and other processed products. This prevalence of fried potatoes, known for their high fat and calorie content, naturally raised suspicions. However, the Harvard researchers went a step further, specifically analyzing the impact of non-fried potato preparations, such as mashed or baked potatoes. To the surprise of many, even these seemingly healthier forms showed a similar statistical link to an increased risk of diabetes. This finding propelled the discussion beyond just the detrimental effects of frying and into the inherent properties of the potato itself.
Unpacking the Potato Paradox: Confounding Factors and Adjustments
Nutritional epidemiology is complex, often grappling with a multitude of confounding variables that can obscure true cause-and-effect relationships. Researchers involved in the Nurses’ Health Study were acutely aware of these challenges. One immediate hypothesis for the observed link was the "meat-and-potatoes" dietary pattern prevalent in many Western cultures. Individuals who consumed more potatoes often also consumed more meat, particularly red and processed meats, which have independently been linked to an increased risk of Type 2 Diabetes. To account for this, the researchers employed sophisticated statistical adjustments, attempting to isolate the effect of potato consumption from that of meat intake. Despite these adjustments, the association between potatoes and an elevated diabetes risk persisted.
Beyond the meat factor, the typical accompaniments to baked and mashed potatoes—butter and sour cream—also presented a potential confounding issue. These high-fat dairy products add significant calories and saturated fat to a meal, components that can influence metabolic health. The research team meticulously attempted to adjust for these additional dietary factors, including the ratio of plant to animal fats in participants’ diets, soda consumption, and the intake of other vegetables. Even after these comprehensive statistical controls, the consistent association between potatoes and diabetes remained, albeit with varying degrees of strength depending on the potato preparation. This rigorous approach underscored the need for a deeper understanding of the potato’s role in glucose metabolism.
Potatoes are primarily a source of carbohydrates, specifically starch. Starchy foods are digested into glucose, which enters the bloodstream and triggers an insulin response. The speed and magnitude of this glucose surge are measured by the Glycemic Index (GI) and Glycemic Load (GL). White potatoes, particularly when baked or boiled and eaten hot, generally have a high GI, meaning they cause a rapid increase in blood glucose levels. This rapid spike requires a quick and substantial insulin release from the pancreas. Over time, frequent and high glycemic load meals can contribute to insulin resistance, a hallmark of Type 2 Diabetes, where the body’s cells become less responsive to insulin. This physiological mechanism provided a plausible biological explanation for the observed epidemiological links, moving the discussion beyond mere correlation to potential causation.
Expanding the Evidence Base: Multiple Cohorts and Persistent Associations
The scientific community rarely accepts the findings of a single study as definitive. By 2015, Harvard researchers had broadened their investigation, integrating data from additional cohorts to corroborate or refute the initial findings. This included the Health Professionals Follow-up Study, an all-male cohort that provided a crucial counterpoint to the all-female Nurses’ Health Study. The results from these diverse populations largely mirrored the earlier findings: a small but consistent increased risk of diabetes was associated with the consumption of baked, boiled, or mashed potatoes.
However, the distinction between potato preparations became increasingly clear and significant. French fries, in particular, consistently emerged as a far more problematic food item, appearing to be nearly five times worse than non-fried potatoes in terms of associated diabetes risk. This stark difference highlighted the profound impact of processing and cooking methods on the health implications of a food.
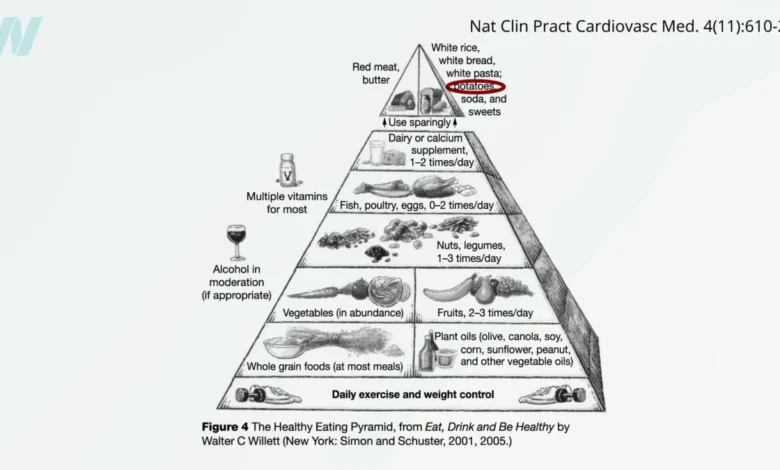
The authors of these comprehensive Harvard studies concluded that while potatoes had traditionally been categorized as a healthy vegetable in most dietary guidelines globally, the accumulating evidence "casts serious doubts on this classification." This was a bold statement, challenging conventional wisdom and prompting a reevaluation of dietary advice. Dr. Walter Willett, then chair of Harvard’s nutrition department and a leading figure in public health, even went a step further in 2007, suggesting that potatoes should be reclassified alongside foods like candy, implying they should be consumed sparingly due to their rapid impact on blood sugar. This provocative comparison underscored the gravity with which these findings were viewed by prominent experts in the field. The implications for public health messaging were substantial, suggesting that a blanket endorsement of potatoes as a "healthy vegetable" might be misleading without careful consideration of preparation methods and overall dietary context.
The Broader Picture: A Meta-Analysis Confirms Trends
To synthesize the growing body of research, a comprehensive meta-analysis of potato consumption and the risk of Type 2 Diabetes was published in 2018. This study combined data from all six prospective studies conducted to date on the topic, providing a more robust statistical assessment than any single study could offer. The meta-analysis, published in Diabetes Care, revealed an approximate 20% increase in diabetes risk associated with each daily serving of potatoes. The researchers concluded that "long-term high consumption of potato…may be strongly associated with increased risk of diabetes."
Despite the strength of this meta-analysis, a critical limitation remained: the vast majority of potatoes consumed across the combined studies were in their fried forms. The researchers acknowledged that they were unable to sufficiently differentiate between the effects of french fries and non-fried potatoes due to data limitations. This inability to disentangle the specific effects meant that the overall 20% increased risk might be heavily skewed by the detrimental impact of fried varieties. Indeed, the analysis showed that even just three servings of french fries per week were associated with nearly a 20% greater risk of Type 2 Diabetes, whereas the associated risk for potatoes in general (which included the fried varieties) was only tiny. This observation strongly suggested that the frying process, and the resulting chemical changes and addition of unhealthy fats, was a primary driver of the observed risks. Deep-fried foods are known to contain advanced glycation end-products (AGEs), harmful compounds formed when sugars react with proteins or fats, particularly during high-temperature cooking. AGEs have been implicated in various chronic diseases, including diabetes and cardiovascular disease, further solidifying the argument against fried potatoes.

Industry Response and Methodological Scrutiny
The accumulating scientific evidence linking potatoes to increased diabetes risk did not go unnoticed by the food industry, particularly those with significant investments in potato products. McCain Foods, a global giant claiming to produce one in three french fries consumed worldwide, generating billions in revenue, publicly challenged some of these conclusions. Their reaction was swift and indicative of the economic stakes involved.
McCain Foods, like other industry players, has the financial capacity to commission and fund scientific reviews and research that may offer alternative interpretations or highlight methodological limitations of studies that cast their products in a negative light. One such industry-funded review, published in the British Journal of Nutrition, cautioned that scientific literature on potatoes should be interpreted with care. It argued that the impact of potatoes on disease risk factors might heavily depend on the broader dietary pattern in which they are consumed. This point is valid and underscores a fundamental challenge in nutritional epidemiology: isolating the effect of a single food item from the synergistic effects of an entire diet.
The Potato Association of America, a scientific organization dedicated to advancing potato research, echoed these sentiments. They frequently reminded the scientific community that observational studies, while crucial for identifying associations, cannot definitively prove cause and effect. They emphasized the difficulty, if not impossibility, of entirely separating the effects of potatoes—whether baked, boiled, or fried—from the overall impact of a generally unhealthy "Standard American Diet" (SAD). This diet, characterized by high intake of processed foods, refined grains, unhealthy fats, and sugars, provides a complex backdrop against which to assess individual food components. It is plausible that individuals who consume more potatoes, especially in Western contexts, might also adhere to less healthy dietary patterns overall, making the potato a marker for an unhealthy diet rather than the sole causal agent.
A Contrasting Perspective: The Iranian Study and Dietary Context
The complexities of dietary patterns and confounding factors reached a critical juncture with the emergence of a seventh prospective study, this time originating from Iran. This study provided a fascinating counter-narrative to the prevailing Western-centric findings. In Iran, the predominant mode of potato consumption is boiling, often as part of traditional stews and alongside a diet rich in whole plant foods, including fruits, vegetables, legumes, and whole grains.
Crucially, the Iranian study found that individuals who consumed more boiled potatoes actually had healthier overall diets. They were more likely to consume greater quantities of whole plant foods, suggesting that in this cultural context, potato consumption was a marker for a more nutritious diet, not a less healthy one. Despite attempts by the researchers to statistically tease out the effects of these other dietary factors, those eating the most boiled potatoes exhibited only half the odds of developing diabetes.
This finding from Iran provided a powerful illustration of the "dietary pattern" argument. It strongly supported the notion that it may be challenging, if not misleading, to completely isolate the health effects of a single food like the potato without considering its cultural and dietary context. When integrated into a diet rich in other healthy components, and prepared without excessive fats or processing, potatoes appear to behave very differently in terms of their health impact. This highlights the importance of cultural variations in diet and how the same food can have different health implications depending on the overall dietary matrix.
Navigating the Nutritional Landscape: Implications for Dietary Guidelines and Consumers
The journey of understanding the potato’s role in diabetes risk culminates in a nuanced perspective. A systematic review published in 2016, preceding the meta-analysis, concluded that there was no "convincing evidence" that the intake of potatoes in general is directly linked to Type 2 Diabetes, provided that other confounding factors are adequately controlled for. This conclusion, while cautiously worded, offered a more optimistic outlook for non-fried potatoes.
The overarching implication for public health and dietary guidelines is clear: context matters immensely. While potatoes themselves are rich in vitamin C, potassium, and fiber (especially when consumed with the skin), their preparation and the company they keep on the plate significantly alter their health profile.
For consumers, the takeaway message is one of moderation and mindful preparation. The scientific consensus strongly suggests that deep-fried potatoes, such as french fries and potato chips, should be limited due to their high glycemic load, unhealthy fats, advanced glycation end-products, and overall association with increased diabetes risk. This recommendation is robust and widely supported across various studies and analyses.
However, for non-fried potatoes—baked, boiled, or mashed without excessive butter, sour cream, or other high-fat additives—the evidence is less condemnatory. When integrated into a balanced diet rich in whole plant foods, as seen in the Iranian study, their consumption may not pose a significant diabetes risk and could even be part of a healthy eating pattern. Factors such as cooling cooked potatoes can even increase their resistant starch content, which has beneficial effects on gut health and blood sugar control.
The ongoing scientific debate underscores the inherent challenges in nutritional epidemiology. Human diets are incredibly complex, and isolating the impact of individual food items is a formidable task. The potato, once a simple and universally accepted staple, now serves as a prime example of how scientific inquiry can reveal layers of complexity, transforming our understanding and prompting a more nuanced approach to dietary recommendations. While the scientific community continues to refine its understanding, the prudent advice remains: enjoy potatoes in their least processed forms, mindful of accompaniments, and always as part of a diverse and balanced diet.







{kind=link}